- Research
- Open access
- Published:
Biphasic anaphylaxis in a Canadian tertiary care centre: an evaluation of incidence and risk factors from electronic health records and telephone interviews
Allergy, Asthma & Clinical Immunology volume 21, Article number: 7 (2025)
Abstract
Background
Our previous 2007 study reported a 19.4% rate of biphasic anaphylaxis in Kingston, Ontario. Since then, few updates have been published regarding the etiology and risk factors of biphasic anaphylaxis. This study aimed to describe the incidence of and predictors of biphasic anaphylaxis in a single centre through a retrospective evaluation of patients with diagnosed anaphylaxis.
Methods
From November 2015 to August 2017, all patients who presented to the emergency department at two hospital sites in Kingston given a diagnosis of “allergic reaction,” “anaphylaxis,” “drug allergy,” or “insect sting allergy,” were evaluated. Patients were contacted sometime after ED discharge to obtain consent and confirm symptoms and timing of the reaction. A trained allergist determined if criteria for anaphylaxis were met and categorized the reactions as being uniphasic, biphasic, or non-anaphylactic biphasic. A full medical review of the event ensued, and each type of anaphylactic event was statistically compared.
Results
Of 138 anaphylactic events identified, 15.94% were biphasic reactions, 79.0% were uniphasic, and 5.07% were classified alternatively as a non-anaphylactic biphasic reaction. The average time of a second reaction was 19.0 h in patients experiencing biphasic reactivity. For biphasic anaphylaxis, the symptom profiles of second reactions were significantly less severe (p = 0.0002) compared with the initial reaction but significantly more severe than non-anaphylactic biphasic events (p < 0.0001).No differences of management were identified between events.
Conclusion
The incidence of biphasic reactions in this cohort was 15.94% and the average second-phase onset was 19.0 h. In biphasic reactivity, it appears that the symptom profile second reaction is less severe compared to the first reaction.
Background
Anaphylaxis is an acute, potentially life-threatening systemic allergic reaction. It is defined as “a serious allergic reaction that is rapid in onset and may cause death” [1]. Many triggers have been identified to cause anaphylaxis, including food, insect stings and medications [2]. The prevalence of anaphylaxis ranges from 0.05 to 3%, with increasing rates of hospitalizations. In the United States, rates of anaphylaxis hospitalizations increased from 20 to 25.1 per million population between 1999 and 2009 [3, 4]. Despite the increasing rates of hospitalizations, fatality rates remain relatively unchanged and rare, constituting less than 1% of total mortality risk [5, 6]. The severity of clinical presentation varies widely. Still, it involves the acute onset of illness and frequently involves the skin and/or mucosa and either respiratory compromise or low blood pressure or end-organ dysfunction [7]. The time course for anaphylaxis can be classified as uniphasic, where a patient experiences a single anaphylactic reaction; protracted, where a patient experiences a single anaphylactic reaction but symptoms persist for a longer duration despite treatment; or biphasic [8]. Standard practice recommendations are observing patients until signs and symptoms have resolved. If the risk for biphasic reactivity or anaphylaxis fatality is determined to be higher, then extended observation for a 6 h or more is appropriate [2]. Furthermore, the World Allergy Organization (WAO) anaphylaxis guidelines are valuable when considering discharge and follow-up among patients treated for anaphylaxis [9]. The WAO recommends that at the time of discharge, patients at risk of another episode of anaphylaxis should be prescribed and taught about self-administration of epinephrine and have a written personalized anaphylaxis emergency action plan and medication identification method [9].
According to the anaphylaxis: a 2023 practice parameter update, biphasic anaphylactic reactions are defined as the recurrence of a reaction or the development of new symptoms 1–48 h after the resolution of the initial presentation without further exposure to the trigger [10]. It is reported to occur in 1–20% of patients [11, 12]. The exact etiology for biphasic reactions remains unclear; however, some known risk factors include a more severe initial presentation of anaphylaxis, necessitating repeated epinephrine doses, wide pulse pressure, unknown anaphylaxis triggers, and cutaneous signs and symptoms [8, 12]. Delayed or underused epinephrine treatment for initial anaphylaxis has been identified as a risk factor for developing biphasic anaphylaxis [13,14,15]. Rapid and complete resolution of acute symptoms has also been related to a decreased risk of developing biphasic reactions [16, 17]. The mainstay of treatment for anaphylaxis is the rapid administration of intramuscular epinephrine. Other important management strategies include supine positioning, supplemental oxygen, and intravenous fluids. Second-line optional treatments include antihistamines, corticosteroids, and bronchodilators, but these agents should never be used in place of epinephrine to manage anaphylaxis [9].
In 2007, we reported an incidence rate of 19% (n = 20) for biphasic reactions where the mean time to onset of the second phase was 10 h (range 2–38 h) in Kingston, Ontario. In 2007, 70% of patients treated for anaphylaxis in the ED received epinephrine [17]. This study aims to provide an update on the incidence of, and potential predictors for, biphasic anaphylaxis in a single centre through a retrospective evaluation of patients with diagnosed anaphylaxis. While this examination of biphasic anaphylaxis in Kingston and its surrounding area involves a small number of patients, it nonetheless provides important insights into an understudied and underreported phenomenon.
Methods
Study Design and Time Period
The Queen’s University and Affiliated Teaching Hospitals Health Sciences Human Research Ethics Board reviewed this study and granted ethical clearance.
All patients with ED visits who were diagnosed with “allergic reaction,” “anaphylaxis,” “drug allergy,” or “insect sting allergy” from November 2015 to August 2017 were evaluated. We first received verbal consent from patients on the phone to complete a survey. Trained study staff reviewed medical records and discussed the allergic event with the participant within two months of occurrence. Using this hybrid data collection method ensured a comprehensive understanding of the allergic event, including the cause and timing of the reaction, symptoms, and any treatment received. Participants were questioned about common allergic symptoms using easy-to-understand language, and the ED records were also consulted, especially when evaluating clinically identifiable symptoms (e.g., tachycardia, hypoxemia). Initial interest in treatment utilized in the ED focused on the collection of data on the progression and sequence of treatment, including the class of treatment. Special attention was given to any symptoms reoccurring after the allergic reaction had completely cleared. After completion, we sent out consent forms and asked them to be signed and returned for documentation purposes, though it was not required for study participation. Patients’ medical records related to the incident were reviewed by a trained allergist, and cases were classified as uniphasic, biphasic, or non-anaphylactic biphasic reactions.
Outcome Measures
Anaphylaxis was defined according to the Canadian Pediatric Surveillance Program (CPSP) as a severe allergic reaction to any stimulus, having sudden onset and generally lasting less than 24 h, involving at least two body systems, with multiple symptoms such as hives, flushing, angioedema, stridor, wheezing, shortness of breath, vomiting, diarrhea, or shock [17]. For a reaction to be labelled “biphasic,” the second-phase reaction must meet the same definition. Recurrence of urticaria or another rash alone was insufficient to qualify as a biphasic reaction. Following the complete resolution of anaphylaxis symptoms, several participants reported the recurrence of single-system reactions (e.g., urticaria alone). For this analysis, the descriptor “non-anaphylactic biphasic reaction” was assigned.
Data Analysis
Statistical analyses were completed using GraphPad Prism 9.
Results
From November 2015 to August 2017, 155 anaphylaxis events were identified, consisting of 148 unique patients, of whom 17 were excluded due to the withdrawal of consent. Eight patients out of 131 experienced two unrelated anaphylactic events during the study period, resulting in 138 anaphylactic events investigated individually. Of the events investigated, 15.94% (n = 22) were biphasic, 5.07% (n = 7) were non-anaphylactic biphasic, and the majority (79.0%, n = 109) were uniphasic (Table 1).
The median age and sex of patients across anaphylactic events were comparable. Among uniphasic, non-anaphylactic biphasic, and anaphylactic biphasic events, there were no significant differences in prior clinical history of anaphylaxis (p = 0.5528) or asthma (p = 0.7483), time to onset of symptoms for first reactions (p = 0.9793) or time to resolution of symptoms for first reaction (p = 0.0677; uniphasic = 3.75 h, non-anaphylactic biphasic = 5.50 h, biphasic = 2.50 h). The mean recurrence time of a second phase reaction was similar (p = 0.9585) between non-anaphylactic biphasic events (20.2 h) and biphasic events (19.0 h). There was also no correlation between time to resolution and recurrence time in this cohort of biphasic events (r = 0.1217, p = 0.6755).
Food was the leading trigger for uniphasic events (43%, n = 47), whereas insect stings (43%, n = 3) and unknown antigens (41%, n = 9) were the most common triggers for non-anaphylactic biphasic and biphasic events, respectively (Table 2). The distribution of triggering antigens, categorized as food, medication, insect stings, miscellaneous, and unknown, is significantly different (p < 0.05) between uniphasic biphasic reactions (Fig. 1). Anaphylactic and non-anaphylactic biphasic reactions had similar distributions of anaphylactic triggers (p = 0.8655).
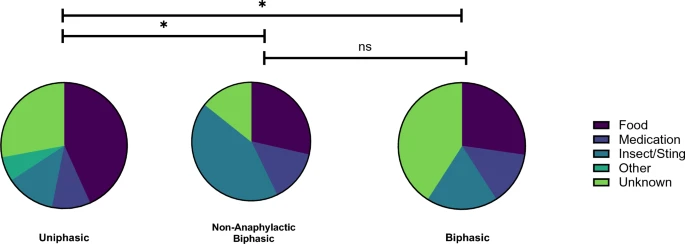
Reaction profiles. The proportion of anaphylactic triggers across the responder groups is represented by pie charts. The reaction profiles significantly differed between uniphasic responders and non-anaphylactic biphasic and biphasic responders (p = 0.0179 and p = 0.0375, 2-way ANOVA with Tukey’s Multiple Comparisons test). Reaction profiles were comparable between non-anaphylactic biphasic and biphasic responders (p = 0.8665, 2-way ANOVA with Tukey’s Multiple Comparisons test)
The initial presenting symptoms were not significantly different for patients with uniphasic or biphasic reactions (p > 0.9080, Fig. 2A).However, among patients experiencing a biphasic reaction, they were characterized with significantly greater (p < 0.05) “other mouth/throat swelling” symptoms than non-anaphylactic biphasic events. Second reactions were less burdensome in terms of symptoms than the initial anaphylactic event for both biphasic (p = 0.0002) and non-anaphylactic biphasic (p < 0.0001) events. Specifically, the symptoms of “wheeze”, “other mouth/throat swelling”, “angioedema”, “lightheadedness/dizzy”, “hoarseness”, and “abdominal pain” were significantly decreased (p < 0.05) in anaphylactic second reaction events compared to the first (Fig. 2B).

Symptoms profiles. A Heat map (left) representing proportional occurrence of specific symptoms across the first anaphylactic response of uniphasic, non-anaphylactic biphasic reaction responders. Biphasic patients were more likely (p = 0.0361, 2-way ANOVA with Tukey’s Multiple Comparisons test) to report “other mouth/throat swelling” than non-anaphylactic biphasics. Heat map (right) representing proportional occurrence of specific symptoms across the second anaphylactic response of non-anaphylactic biphasic and biphasic responders. The secondary anaphylactic reaction of biphasics had significantly less symptoms (p < 0.0001, 2-way ANOVA with Tukey’s Multiple Comparison’s test) than non-anaphylactic biphasics. C Graph displaying the proportion of symptoms experienced by biphasic responders comparing their first and second anaphylaxis reactions. There were six symptoms which were significantly decreased in biphasic responders’ second (red) reaction vs first (blue)
The management of the first anaphylactic reaction was similar in all groups, with a comparable average number of drugs used, including epinephrine, beta-agonists, histamine (H)1 and H2 antagonists, and corticosteroids (Table 3). Most patients received one or two doses of epinephrine for their first reaction; however, two patients received three and four doses for the biphasic events, respectively. Only four events of biphasic anaphylaxis were treated with epinephrine, all requiring only one dose. The average number of medications used to manage the second reaction for biphasic events was significantly greater than for non-anaphylactic biphasics (p = 0.0289). Compared with the initial reactions, second reactions were generally managed with less medication, including epinephrine (p < 0.005), for both anaphylactic (p < 0.0001) and non-anaphylactic (p < 0.0012) biphasic reactions (Fig. 3).

Drugs and Epinephrine Usage. Total Number of Drugs Used (top): The number of drugs used to manage first (red) and second (blue) reactions in biphasic and non-anaphylactic biphasic reactors. For both responder groups, significantly fewer drugs were used to treat their second reaction than the first reaction (p < 0.05, Mann–Whitney test). Epinephrine Usage (bottom): The proportion of non-anaphylactic and biphasic patients who received epinephrine in managing their first and second reactions. For both responder groups, a significantly smaller proportion of patients were administered epinephrine for their second reaction (p < 0.05, Mann–Whitney test)

Flowchart depicting Epinephrine Usage, Doses, and Timings. 138 anaphylactic events were sub-categorized into uniphasic, non-anaphylactic biphasic, and biphasic events. Patients who received epinephrine in each group were identified, and sub-analyses of epinephrine dosage and timing of dose administration relative to ED arrival were conducted. No significant differences were found between the first epinephrine dosage across each responder group (p = 0.9179, Kruskall-Wallis test). Among patients who received their first dose of epinephrine before ED arrival, there was no significant difference in the time between the first dose administration and ED arrival for uniphasic, non-anaphylactic biphasic, and biphasic responders (p = 0.6283, Kruskall-Wallis test). Similarly, among patients who received their first dose of epinephrine after ED arrival, there was no significant difference in the time between ED arrival and the first dose administration for uniphasic, non-anaphylactic biphasic, and biphasic responders (p = 0.4787, Kruskall-Wallis test). The timing of epinephrine administration and ED arrival was comparable among the responder groups (p > 0.05, Mann–Whitney test)
In this cohort, 80% of cases (n = 111) were treated with at least one dose of epinephrine in response to their first anaphylactic event (Fig. 4). The exact time and dose of epinephrine used was known and reported for 90 cases by either the ED, Emergency Medical Services (EMS) or by the patient themselves. There was no significant difference in the average epinephrine dose administered to patients experiencing an initial anaphylactic event (p = 0.9179; Fig. 4). Overall, 46.7% (n = 42) received their first epinephrine dose before arriving in the ED, and 53.3% (n = 48) received their first epinephrine dose after arriving in the ED (Fig. 4). There was no significant difference between the responder groups (e.g., uniphasic vs non-anaphylactic biphasic vs biphasic) groups (p > 0.05) in the mean time between first dose of epinephrine and ED arrival. Within each of the responder groups, there was no significant difference in the time between epinephrine administration and ED arrival for those patients who received epinephrine before ED arrival or after (p > 0.05). The average time to first epinephrine treatment before ED arrival was 30.5 min across groups and 36.4 min when received after ED arrival (Fig. 4).
Discussion
Interpretation of Findings
Biphasic anaphylaxis has a wide range of reported incidences, and in our current study, it was 16%. tThe mean time of second phase reaction was 19.0 h after the first reaction. However, it is relevant to recognize the lack of significant difference between the timing of recurrence between biphasic and non-anaphylactic biphasic events (19.0 vs 20.2 h) as well as the number of second phase reactions that started in less than 8 h (31.8% vs 28.6%). Second reactions had less severe symptom profiles and a correspondingly lower number of medications used for both anaphylactic and non-biphasic events. We found no significant differences in epinephrine administration between all three types of responders, including timing related to ED arrival. The time for the administration of a first dose of epinephrine was comparable whether it was received before or after ED arrival (between 30 and 37 min). The time of first epinephrine administration once a patient arrived in ED at our site was comparable to other clinical practices. Cha et al. reported that epinephrine was administered within 30 min of hospital arrival for 52.6% of patients, while the remaining 47.4% received epinephrine after 30 min or more [18]. There are many factors that may influence the speed of first epinephrine administration, both before and after hospital admission, which are not captured in our study, though they warrant a closer examination.
Interestingly, most biphasic events (80.0%) received a first dose of epinephrine after ED arrival and were more likely to receive subsequent doses, suggesting that delayed administration of epinephrine may have played a role in biphasic anaphylaxis. We did find a statistically significant difference in the distribution of antigens that caused anaphylaxis between the uniphasic with non-anaphylactic biphasic events responders (p = 0.0179) and anaphylactic biphasic responders (p = 0.0375). More specifically, 41% of patients who developed biphasic anaphylaxis had reactions to an unknown trigger (n = 9). This is in keeping with a study that identified unknown trigger as a risk for biphasic reactions [19]. Kraft et al. used data from the European Anaphylaxis Registry to analyze possible risk factors of biphasic anaphylaxis. They analyzed a cohort of 435 cases of biphasic anaphylaxis and compared them with 8736 uniphasic reactions. The authors also saw no difference between the main groups of elicitors of anaphylaxis such as food, drugs and insects. However, they also saw that peanut, and to a lesser extent tree nut, was associated with a higher rate of biphasic anaphylaxis; 9.6% of the reactions were biphasic [20].
Comparison to Previous Studies
In our 2007 study, the incidence of biphasic reactions in Kingston, Ontario, Canada, was 19%, compared to 16% in our current study. The mean time for the occurrence of the second-phase reaction was 19.0 h (range 0.5–72 h), which is longer than the previously reported window of 10 h (range 2–38 h) [17]. Only 31.8% of biphasic events started the second phase less than 8 h after the initial reaction. This supports the results from a study where the interval for the second phase ranged from 4.5 to 29.50 h and another by Lee et al., which reported that approximately half of biphasic reactions occur within 6–12 h [19, 21]. Lieberman et al. also suggested this, concluding that second-phase reactions can occur up to 72 h following the initial reaction [22]. Our study did report a higher incidence of biphasic anaphylaxis compared to other studies, such as the 2019 meta-analysis by Kim et al. (6.5%) and the 2020 systematic review by Chu et al. (3.65%), which is likely a reflection of the inherent sample bias from our single-center study [23].
The risk factors for developing biphasic anaphylactic reactions remain unclear. Previous studies showed that delayed or repeated administration of epinephrine is associated with biphasic reactions [24]. Our study found that 80.0% of patients experiencing a biphasic reaction had their first dose of epinephrine in the ED and 31.6% of biphasic responders required subsequent doses of epinephrine. This finding is consistent with the findings of Liu et al. who found that 19% of patients with biphasic reactions required two doses of epinephrine. This group also found that a biphasic course was associated with an ED setting of the first epinephrine dose (OR 3.72; 95% CI 1.36–10.14) [25].
Rapid and complete resolution of acute symptoms has also been related to a decreased risk of developing biphasic reactions [16, 17]. In this study, we did not find a correlation between time to resolution and recurrence time in this cohort of biphasic events (r = 0.1217, p = 0.6755). On average, initial anaphylactic events were resolved within 6 h for uniphasic and non-anaphylactic biphasic events whereas biphasic events took longer, at 9.5 h. This finding conflicts with our 2007 report, whereby the biphasic reactors, however, took significantly longer to resolve their initial symptoms than uniphasic reactors (133 vs 112 min; P = 0.03) [17].
We also examined the role of corticosteroids; theoretically, their anti-inflammatory and gene expression modulation properties counteract the process of anaphylaxis, though systematic reviews of the literature do not support their role in preventing biphasic responses even as an adjunctive therapy [2, 26]. In our cohort, similar rates of corticosteroid usage were observed between all groups. This appears to be consistent with the literature suggesting that corticosteroids do not prevent biphasic anaphylaxis [2, 27].
Strengths and Limitations
In our study, the timing of biphasic symptoms relied on a chart review with retrospective patient-reported data. Therefore, the consistency of the data may be limited, and recall bias may impact the symptoms reported by the participants. However, clinical definitions were used to identify patients with anaphylaxis. Another weakness is the limited scope of the data, as only a single centre was assessed. While our ED serves patients in Kingston and the surrounding area, our findings may be limited to our own tertiary care centre and the region it serves. Further, this study could not assess anaphylactic reactions that occurred in the community that were not treated by the ED, and so the results of this study are potentially biased by selection of severe anaphylaxis that would present to the ED. This study did not directly assess the impact of epinephrine administration timing. A surrogate for those data was whether epinephrine was administered pre- or post-ED arrival, but high-quality evidence on outcomes when epinephrine is given within 30 min after onset of symptoms is desperately needed. Finally, given that almost half of the patients who had biphasic reactions were related to unknown triggers, there is a possibility that patients were re-exposed to their trigger and subsequently developed a second uniphasic anaphylactic reaction.
Research and Clinical Implications
The mean length of time between reactions in biphasic anaphylaxis, shown in this study to be 19.0 h, raises concerns about prolonging the monitoring period following primary reactions up to 10 h compared to the current usual monitoring period between 4 and 8 h. Extending observation periods can be difficult to achieve in busy EDs and may not be economically advantageous in some circumstances (e.g., resolved anaphylaxis with low risk of biphasic anaphylaxis), and so alternative solutions should be considered, such as patient education, facilitating access to emergent medical care, and prescribing an epinephrine autoinjector at discharge [28]. Similarly, our study noted that most biphasic responders received their first dose of epinephrine after arriving at the ED. However, the reasons for their delay in administration and associated circumstances require further inquiry.
Conclusion
Biphasic reactions remain poorly defined regarding incidence, features, and predictors. Our study, with its specific population of patients from Kingston, ON, showed that biphasic anaphylaxis occurred in 16% of patients with anaphylaxis reporting to the ED. The onset of the second phase reaction was longer than expected, with an average of 19 h, with only 31.8% experiencing symptoms less than 8 h following the initial reaction. Patients with biphasic reactions experienced a prolonged duration of symptoms following their initial reaction. Further larger studies are needed to explore possible predictors and the relation of delayed epinephrine and corticosteroid administration with the occurrence of second-phase reactions.
Availability of data and materials
The datasets generated and analysed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Abbreviations
- ICON:
-
International Consensus on Anaphylaxis
- Ig:
-
Immunoglobulin
- ED:
-
Emergency department
- HSREB:
-
Health Sciences Human Research Ethics Board
- CPSP:
-
Canadian Pediatric Surveillance Program
- EMS:
-
Emergency Medical Service
- H:
-
Histamine
References
Sampson HA, Muñoz-Furlong A, Campbell RL, Adkinson NF, Bock SA, Branum A, et al. Second symposium on the definition and management of anaphylaxis: summary report—second national institute of allergy and infectious disease/food allergy and anaphylaxis network symposium. J Allergy Clin Immunol. 2006;117(2):391–7.
Shaker MS, Wallace DV, Golden DBK, Oppenheimer J, Bernstein JA, Campbell RL, et al. Anaphylaxis-a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. J Allergy Clin Immunol. 2020;145(4):1082–123.
Yu JE, Lin RY. The epidemiology of anaphylaxis. Clinic Rev Allerg Immunol. 2018;54(3):366–74.
Tuttle KL, Wickner P. Capturing anaphylaxis through medical records: are ICD and CPT codes sufficient? Ann Allergy Asthma Immunol. 2020;124(2):150–5.
Jerschow E, Lin RY, Scaperotti MM, McGinn AP. Fatal anaphylaxis in the United States 1999–2010: temporal patterns and demographic associations. J Allergy Clin Immunol. 2014;134(6):1318-1328.e7.
Turner PJ, Jerschow E, Umasunthar T, Lin R, Campbell DE, Boyle RJ. Fatal anaphylaxis: mortality rate and risk factors. J Allergy Clin Immunol Pract. 2017;5(5):1169–78.
Manivannan V, Decker WW, Stead LG, Li JTC, Campbell RL. Visual representation of National Institute of Allergy and Infectious Disease and Food Allergy and Anaphylaxis Network criteria for anaphylaxis. Int J Emerg Med. 2009;2(1):3–5.
Douglas DM, Sukenick E, Andrade WP, Brown JS. Biphasic systemic anaphylaxis: an inpatient and outpatient study. J Allergy Clin Immunol. 1994;93(6):977–85.
Cardona V, Ansotegui IJ, Ebisawa M, El-Gamal Y, Rivas MF, Fineman S, et al. World Allergy Organization Anaphylaxis Guidance 2020. World Allergy Organization Journal [Internet]. 2020 Oct 1 [cited 2023 Jan 11];13(10). Available from: https://www.worldallergyorganizationjournal.org/article/S1939-4551(20)30375-6/fulltext
Golden DBK, Wang J, Waserman S, Akin C, Campbell RL, Ellis AK, et al. Anaphylaxis: a 2023 practice parameter update. Ann Allergy Asthma Immunol. 2024;132(2):124–76.
Tole JW, Lieberman P. Biphasic anaphylaxis: review of incidence, clinical predictors, and observation recommendations. Immunol Allergy Clin North Am. 2007;27(2):309-26. viii.
Oya S, Nakamori T, Kinoshita H. Incidence and characteristics of biphasic and protracted anaphylaxis: evaluation of 114 inpatients. Acute Med Surg. 2014;1(4):228–33.
Lee JM, Greenes DS. Biphasic anaphylactic reactions in pediatrics. Pediatrics. 2000;106(4):762–6.
Lertnawapan R, Maek-a-nantawat W. Anaphylaxis and biphasic phase in Thailand: 4-year observation. Allergol Int. 2011;60(3):283–9.
Alqurashi W, Stiell I, Chan K, Neto G, Alsadoon A, Wells G. Epidemiology and clinical predictors of biphasic reactions in children with anaphylaxis. Ann Allergy Asthma Immunol. 2015;115(3):217-223.e2.
Brady WJ, Luber S, Carter CT, Guertler A, Lindbeck G. Multiphasic anaphylaxis: an uncommon event in the emergency department. Acad Emerg Med. 1997;4(3):193–7.
Ellis AK, Day JH. Incidence and characteristics of biphasic anaphylaxis: a prospective evaluation of 103 patients. Ann Allergy Asthma Immunol. 2007;98(1):64–9.
Cha LMJ, Lee WS, Han MY, Lee KS. The timely administration of epinephrine and related factors in children with anaphylaxis. J Clin Med. 2022;11(19):5494.
Lee S, Bellolio MF, Hess EP, Erwin P, Murad MH, Campbell RL. Time of onset and predictors of biphasic anaphylactic reactions: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2015;3(3):408-416.e2.
Kraft M, Scherer Hofmeier K, Ruëff F, Pföhler C, Renaudin JM, Bilò MB, et al. Risk factors and characteristics of biphasic anaphylaxis. J Allergy Clin ImmunolIn Pract. 2020;8(10):3388–33956.
Brazil E, MacNamara AF. “Not so immediate” hypersensitivity–the danger of biphasic anaphylactic reactions. J Accid Emerg Med. 1998;15(4):252–3.
Lieberman P. The risk and management of anaphylaxis in the setting of immunotherapy. Am J Rhinol Allergy. 2012;26(6):469–74.
Kim TH, Yoon SH, Hong H, Kang HR, Cho SH, Lee SY. Duration of observation for detecting a biphasic reaction in anaphylaxis: a meta-analysis. Int Arch Allergy Immunol. 2019;179(1):31–6.
Fineman S, Dowling P, O’Rourke D. Allergists’ self-reported adherence to anaphylaxis practice parameters and perceived barriers to care: an American College of Allergy, Asthma, and Immunology member survey. Ann Allergy Asthma Immunol. 2013;111(6):529–36.
Liu X, Lee S, Lohse CM, Hardy CT, Campbell RL. Biphasic reactions in emergency department anaphylaxis patients: a prospective cohort study. J Allergy Clin Immunol Pract. 2020;8(4):1230–8.
Lieberman P, Nicklas RA, Randolph C, Oppenheimer J, Bernstein D, Bernstein J, et al. Anaphylaxis–a practice parameter update 2015. Ann Allergy Asthma Immunol. 2015;115(5):341–84.
Liyanage CK, Galappatthy P, Seneviratne SL. Corticosteroids in management of anaphylaxis; a systematic review of evidence. Eur Ann Allergy Clin Immunol. 2017;49(5):196–207.
Shaker M, Wallace D, Golden DBK, Oppenheimer J, Greenhawt M. Simulation of health and economic benefits of extended observation of resolved anaphylaxis. JAMA Netw Open. 2019;2(10): e1913951.
Acknowledgements
The authors would like to thank the Emergency Department at Kingston Health Sciences Centre for their support through patient referrals. The authors would like to recognize the contributions of Leila Alenazy and Grace Yin in the early stages of this project.
Funding
Pfizer Canada.
Author information
Authors and Affiliations
Contributions
LH and SL performed the data analysis and prepared the manuscript. HB and AB administered telephone surveys and collected data following chart review. EB and SG provided clinical expertise and reviewed the manuscript. AKE was involved in all aspects of this study.
Corresponding author
Ethics declarations
Conflict of interest
AKE has participated in advisory boards for ALK Abello, AstraZeneca, Bausch Health, LEO Pharma, Miravo, Merck, Novartis, has been a speaker for ALK Abello, AstraZeneca, Bausch, Miravo, Medexus, Mylan, Novartis, Pfizer, Sanofi, Stallergenes Greer and Regeneron. Her institution has received research grants from ALK Abello, Aralez, AstraZeneca, Bayer LLC, Medexus, Novartis, Sanofi and Regeneron. She has also served as an independent consultant to Bayer LLC, Pharming, and Regeneron. At the time of submission she is the President of the Canadian Society of Allergy and Clinical Immunology (CSACI).
Ethical approval and consent to participate
This study was reviewed and granted ethical clearance by the Queen’s University and Affiliated Teaching Hospitals Health Sciences Human Research Ethics Board. All study participants consented to participate.
Consent for publication
All study participants consented for publication of these study findings.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ellis, A.K., Hossenbaccus, L., Linton, S. et al. Biphasic anaphylaxis in a Canadian tertiary care centre: an evaluation of incidence and risk factors from electronic health records and telephone interviews. Allergy Asthma Clin Immunol 21, 7 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s13223-024-00919-2
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s13223-024-00919-2