- Review
- Open access
- Published:
Food oral immunotherapy
Allergy, Asthma & Clinical Immunology volume 20, Article number: 82 (2024)
Abstract
Food oral immunotherapy (OIT) is an option for the treatment of immunoglobin E (IgE)‐mediated food allergy that involves administering gradually increasing doses of an allergenic food over time (under medical supervision) with the goal of desensitizing an individual to the food allergen. Current Canadian clinical practice guidelines for OIT recommend this form of therapy as an option in patients with food allergy. The intervention should be prioritized in the infant and toddler population, in which it is particularly well tolerated and can lead to sustained unresponsiveness (also sometimes referred to as remission). In this article, we provide an overview of OIT and discuss the role non-allergist clinicians can play in caring for patients undergoing OIT.
Key take-home messages
-
OIT is a safe and effective treatment option for IgE-mediated food allergy.
-
Early OIT, especially during infancy and preschool age, appears to be safer and more effective compared to starting OIT in older children.
-
OIT is disease-modifying when started early. It should therefore be provided as a management option for families of infants who have failed primary prevention of food allergy. Referral to an allergist who offers this form of therapy should be considered.
-
Choosing OIT as a treatment option involves shared decision-making between the patient, family, and allergist. Goals of treatment are important to establish at the start of treatment.
-
Patients in clinical trials undergoing OIT may experience more allergic reactions than those treated with placebo, but reactions tend to decrease in frequency and severity as treatment progresses. The risk of reactions with avoidance in the real world may be as high as with OIT.
-
For higher-risk patients, a safer approach is an initial phase of SLIT to bypass OIT build-up.
-
Non-allergist clinicians (i.e., family physicians, pediatricians) can play an important role in identifying patients who may benefit from OIT. They can also be instrumental in helping patients undergoing OIT prevent and manage possible adverse reactions during therapy.
Introduction
Food oral immunotherapy (OIT) is an approach to the treatment of patients with immunoglobin E (IgE)‐mediated food allergy (see IgE-mediated Food Allergy article in this supplement) [1]. It consists of daily ingestion of the offending food allergen (food dosing), starting below a patient’s threshold dose (i.e., the minimum amount of food protein that would elicit an allergic reaction), and increasing the dose over time with a goal of increasing clinical tolerance to that food [2]. For infants with a diagnosis of new food allergy, OIT should be discussed as a treatment option, and if it is not offered by the patient’s allergist, referral to an allergist who provides this form of therapy should be considered. OIT may also be an option for older children and adults as part of their food allergy management. Recently published Canadian clinical practice guidelines for OIT favorably recommend the use of OIT outside the research setting [2]. Although these guidelines also suggest that OIT may be an option for adults with food allergy, it is not currently offered to adults by the majority of Canadian allergists. This article will define key terms and concepts related to OIT as well as review the safety and efficacy of this form of therapy and the role of non-allergist clinicians in managing patients on OIT.
Key concepts and definitions related to OIT
Definitions of key terms and concepts related to OIT are provided in Table 1 and Fig. 1. The initial goal of OIT is clinical desensitization, which is defined as an increase in the threshold of allergen required to cause an allergic reaction while on therapy (i.e., with regular ingestion of the allergen) [3]. Longer term goals include sustained unresponsiveness (also sometimes referred to as remission) and, ideally, oral or immunological tolerance. Sustained unresponsiveness is defined as a state in which the patient who is desensitized can stop eating the food for a period of time after OIT has been discontinued and remains non-reactive when the food allergen is re-ingested. Underlying immune mechanisms for desensitization and sustained unresponsiveness are illustrated and described at the bottom of Fig. 1.

Reproduced from Bégin et al. 2020 [2]. Creative Commons license: https://creativecommons.org/licenses/by/4.0/ No changes have been made to the figure
Typical phases of an OIT protocol.
Figure 1 illustrates the typical phases of an OIT protocol. Generally, the first step of OIT involves an initial rapid dose-escalation phase where the food allergen is introduced under medical supervision to identify a dose below the reactivity threshold to begin daily home dosing. The amount of the daily home dose is then increased every few weeks during medically supervised up-dosing visits (i.e., build-up phase) until a predefined target maintenance dose is reached. During the maintenance phase, home OIT dosing continues daily at the same dose to: (1) maintain desensitization, and (2) to induce sustained changes in the immune response to the allergen over time. Patients generally remain on their maintenance dose for a prolonged period with follow-up clinic visits to monitor for safety, assess immunologic response and/or protection on and off therapy with oral food challenges (OFCs) (a procedure in which the patient eats the suspected allergenic food in incrementally increasing doses, up to a serving size, under close medical supervision).
Immune changes with OIT are expected to plateau over 3–5 years. These include a decrease in T helper 2 (TH2) responses and increased regulatory T cell responses, resulting in an initial increase followed by a decrease in allergen-specific IgE and the production of allergen-neutralizing immunoglobulin G4 (IgG4) antibodies [2]. Sustained benefit in infants and toddlers is likely driven by the decrease in specific IgE levels which tend to decrease below pre-OIT levels, as well as increased IgG4. In older patients, sustained benefits are likely mostly driven by the increase in IgG4 since specific IgE tend not to decrease below pre-OIT levels. Based on patient objectives and preferences, some may wish to continue regular dosing indefinitely to retain full protection. Another option is to discontinue daily dosing for a period of time (e.g., weeks or months) and perform an OFC in clinic to assess the extent of sustained protection off therapy.
Benefits of OIT
Several clinical trials and meta-analyses have found substantial benefits for patients undergoing OIT [4,5,6,7,8,9]. Desensitization rates reported in OIT studies, including phase 3 clinical trials, generally range between 67 and 92%, and depend on the definition used (e.g., tolerance to 1 vs. 16 peanuts) and the patient population studied [6,7,8,9]. While desensitized, the patient is protected against accidental exposures with amounts below their new reactivity threshold. In some cases, it may allow the patient to introduce the allergen in their regular diet. In practice, desensitization even against small amounts can translate into a significant impact on quality of life (QoL) for patients. Compared to both pre-OIT treatment and placebo-treated subjects, studies have found improved QoL and less anxiety in subjects completing OIT [10,11,12,13]. In a prospective cohort study of parents of 191 food-allergic children 4–12 years of age undergoing OIT, QoL improved significantly upon reaching OIT maintenance on multiple dimensions including emotional impact (p = 0.001), food anxiety (p < 0.001), social and dietary limitation (p < 0.001), and global score (p < 0.001) [13].
The other benefit from OIT over time is to promote sustained tolerance to the allergen. Compared to placebo, OIT increases the chance of achieving sustained unresponsiveness to the allergen by seven-fold [5]. This benefit is most evident in the infant/toddler population when there is still a potential for outgrowing the allergy. The odds of achieving sustained unresponsiveness with OIT is inversely correlated with age and specific IgE levels, reaching up to 78% for peanut in infants and toddlers under 4 years of age [7]. An important finding from IMPACT–an international randomized controlled trial (RCT) assessing long-term outcomes of peanut OIT in peanut-allergic children 1–3 years of age–was sustained unresponsiveness being highly enhanced in the youngest toddlers with low baseline peanut sIgE (71% sustained unresponsiveness for screening age 12.0–23.9 months vs. 35% for age 24.0–35.9 months vs. 19% for age 36.0–47.9 months; p = 0.013) [9]. In this trial, the definition for sustained unresponsiveness was a very long period of treatment cessation (discontinuation of OIT for 26 weeks).
While older patients with severe allergy are not expected to achieve sustained unresponsiveness with OIT, they can still attain sustained benefits from the treatment. In fact, even if they do not tolerate the full OFC, studies have shown that the vast majority of patients do tolerate higher doses of allergen after discontinuing therapy compared to their OFCs at study entry [14]. This likely reflects protection from allergen-specific IgG4, which are produced as a result of OIT regardless of age.
The benefits of OIT have also been confirmed in real-world studies. The Canadian Preschool Peanut Oral Immunotherapy (CPP-OIT) project found that, of 117 toddlers (mean age = 26 months) who successfully completed peanut OIT and underwent a cumulative 4000-mg follow-up OFC, 78.6% had a negative challenge and 98.3% tolerated a cumulative dose of > 1000 mg [15]. Another recent Canadian real-world study found that low-dose sesame OIT (200 mg maintenance dose) was safe and led to the successful desensitization of 18 of 21 (85%) preschoolers with sesame allergy as measured on their exit OFC [16]. Only one patient (3.6%) required epinephrine during the build-up phase, and no patients required epinephrine in the maintenance phase.
It should be noted that the preschool-age population appears to have better outcomes with OIT than older children, with higher rates of desensitization and a lower risk of adverse events, including anaphylaxis [6, 17, 18].
Safety of OIT
Overall, OIT is considered safe, although adverse reactions to food doses can occur. Mild-to-moderate cutaneous or gastrointestinal symptoms, such as local urticaria, oropharyngeal pruritus and abdominal pain, are common. Severe systemic reactions, such as anaphylaxis, are less common but can also occur. A systematic review and meta-analysis of 12 studies including primarily older children (median age across trials was 8.7 years) found a higher rate of anaphylaxis (16.5%) during peanut OIT compared with avoidance (2.7%) [19]. As mentioned earlier, side effects to OIT are more common in the older population [6, 9, 17, 18]. However, it is important to note that systematic reviews typically use the placebo arms of clinical trials to estimate safety risks with avoidance, but a more clinically relevant comparator is the real-world risk of avoidance as demonstrated in prospective data from a 3-year follow-up of children (median age at follow-up was 11.5 years) with double-blind, placebo-controlled OFC-confirmed peanut allergy [20]. What was most concerning from this real-world data was not only that 29% experienced severe symptoms, but moreover none of the reactions were treated with epinephrine.
In a meta-analysis by the Global Allergy and Asthma European Network (GA2LEN) Food Allergy Guideline Group that included 36 RCTs involving 2126 participants (primarily children), OIT was not associated with a significant increase in adverse or severe reactions in peanut allergy; however, an increase in mild adverse reactions (primarily oral pruritus and gastrointestinal pain) in cow’s milk and hen’s egg allergy was observed [5].
The safety of peanut and tree nut OIT in preschoolers has been established in the real-world Canadian population [21, 22]. Soller et al. administered peanut OIT to 270 preschoolers in the real-world setting and found treatment to be safe for the majority of patients, with 71.2% of reactions during build-up being mild, 0.2% of reactions being severe, 2.2% of reactions requiring epinephrine, and a low dropout rate (10%) [21]. Another real-world, multicentre analysis of tree nut OIT in 97 preschoolers found OIT to be safe and tolerable [22]. The majority of patients experienced mild-to-moderate reactions during the build-up phase (70.6%), 2% received epinephrine and no serious grade 3 or 4 reactions were reported. A recent Canadian real-world study found the safety of preschool peanut OIT or peanut OIT using a slower build-up schedule to be comparable to that of subcutaneous immunotherapy (SCIT) (used for the treatment of common allergic conditions resulting from environmental/aeroallergens–see Allergen Immunotherapy article in this supplement [23]) despite differences in OIT protocols used and age groups studied [24].
An important factor to consider prior to starting OIT is the risk of eosinophilic esophagitis (EoE; see article on EoE in this supplement [25]). The rate of EoE in OIT is estimated to be between 0.5 and 5% [26]. However, it is important to note that children with food allergies are already at risk of EoE at baseline, although the risk appears to be lower in infants and toddlers [21]. At present, it remains unclear whether OIT causes EoE, or rather “unmasks” it in patients who had pre-existing, undiagnosed esophageal eosinophilia [27,28,29,30,31,32]. Additional studies are required to further evaluate the relationship between OIT and EoE. Until then, a practical approach based on shared decision-making for continuing OIT when it has unmasked EoE can be considered [33].
It is also important to consider cofactors that alter immune homeostasis or allergen absorption, such as viral infections, fever, exercise, use of non-steroid anti-inflammatory drugs (NSAIDs), hormonal changes and evening ingestion/dosing, as these may play a role in triggering an adverse reaction to an OIT dose that is otherwise usually tolerated [34, 35]. In general, avoidance of physical activity for at least 1 h before and 3 h after intake of a food allergen is recommended [34]. In those with a fever or infectious condition, suspension or reduction of the OIT food dose for a few days is generally advised.
Infant OIT for failed primary prevention
Primary prevention of food allergy has become an important public health goal (see Primary Prevention of Food Allergy: Beyond Early Introduction article in this supplement) [36]. It involves early introduction of allergenic foods in high-risk infants (i.e., those with mild to moderate atopic dermatitis, a family history of atopy in either or both parents, or those with one known food allergy) to reduce the risk of development of food allergy [37]. None of the current primary prevention guidelines provide detailed advice for managing infants who experience failed primary prevention [37,38,39], beyond the implication that it results in the need for avoidance of the allergenic food(s) and carrying an epinephrine autoinjector.
Although population-level data describes predictors of which infants are most likely to outgrow food allergy [40], clinically an allergist cannot reliably predict whether an infant is likely to outgrow food allergy as there will be outliers. At present, novel biomarkers for predicting which individual infants will outgrow their food allergy are either not precise enough or not yet ready for use outside the research setting [41].
In early 2017, a seminal study published by Vickery et al. demonstrated for the first time that peanut OIT was very effective in peanut-allergic preschoolers aged 9–36 months (n = 40) who were randomized to either low-dose (300 mg) or high-dose (3000 mg) peanut OIT over a median of 29 months (including a 10.5-month build-up period) [7]. The desensitization rate was 85% in the low-dose group and 76% in the high-dose group. Furthermore, 78% of toddlers achieved sustained unresponsiveness to peanut 4 weeks after discontinuing OIT and reintroducing peanut into the diet. Predominantly mild symptoms, such as abdominal pain, skin/oral pruritus, nausea, sneezing/congestion and hives, were reported and there was one moderate reaction requiring epinephrine [7].
A recent Canadian study comparing OIT in infants (aged < 12 months) versus non-infant preschoolers (aged 12–70 months) found OIT to be equally effective in both groups, yet safer in infants [42]. As evidence of how important the outcome of safety is to stakeholders, a recently published international Delphi consensus study (“COMFA”) of 778 participants from 52 countries (which included patients and caregivers) found that only two outcomes achieved consensus for inclusion as “core” outcomes in future food allergy clinical trials and observational studies: allergic symptoms (i.e., safety) and QoL [43, 44].
As discussed above, IMPACT found that the earlier OIT is started in childhood, the greater the likelihood of sustained unresponsiveness or tolerance [9]. Also, the earlier OIT is initiated, the more cost effective it may be [45], with the added benefit of improving QoL considerably earlier than if it is deferred until a child is older [46].
Based on personal preferences, families of infants failing primary prevention may still choose avoidance. However, in the current era of shared decision-making, families should be informed that this may result in a permanently missed opportunity to induce sustained unresponsiveness. They should be made aware of infant OIT as a management option for failed primary prevention [47] and referred to an allergist if they are interested in pursuing this form of therapy. In areas where access to an allergist is limited, e-consultations can be used to determine the best course of action while waiting for an in-person consultation.
OIT guidelines
Several allergy organizations have released guidelines on OIT [48], but the most relevant for Canadian clinicians are those published by the European Academy of Allergy and Clinical Immunology (EAACI) [49] and the Canadian Society of Allergy and Clinical Immunology (CSACI) [2] (Table 2). Both the EAACI and CSACI guidelines emphasize the importance of shared decision-making with patients and caregivers before initiating, and during, OIT. OIT is considered a personalized treatment that needs to be adapted to the patient’s context, individual risks and benefits, goals and objectives for therapy, eating habits, experience, and motivation.
The EAACI recommends waiting for the allergy to resolve naturally before starting OIT, and only recommends it from the age of 4–5 year. It should be noted, however, that the EAACI recommendations were published in 2018 before more recent evidence from randomized trials such as IMPACT [9] became available showing greater efficacy of OIT when started at earlier preschool ages. Also, the EAACI only recommends OIT for cow’s milk, egg and peanut allergy, and does not recommend OIT for adults [49]. In contrast, the CSACI recommends OIT for all foods and for all patients (children and adults) wishing to receive it, provided that there are no contraindications to therapy and that patients and caregivers have a clear understanding of individual risks and benefits [2].
According to both guidelines, uncontrolled asthma and pregnancy are absolute contraindications for OIT, while active severe atopic dermatitis, pre-existing EoE, heart disease, and the use of beta-blockers or angiotensin-converting enzyme (ACE) inhibitors are relative contraindications based on clinical judgement, provider expertise, and shared decision-making [2, 49]. Patient- or caregiver-specific contexts that may jeopardize the safe administration of therapy must also be assessed. For example, failure to adhere to the OIT protocol and attend regular appointments and/or the inability to recognize and treat severe reactions (e.g., reluctance to use epinephrine) constitute contraindications for OIT [2, 49].
Both the CSACI and EAACI guidelines specify that allergists practicing OIT must have expertise in this type of care as well as infrastructure that allows for the regular and personalized follow-up of patients, the performance of OFCs, and the management of anaphylaxis [2, 49]. Informed consent that clearly specifies the risks and benefits of OIT must be obtained before initiating therapy.
Access to OIT in Canada
There are disparities in accessing OIT in Canada, which are further exacerbated by increasing demand, the lack of specialized care in both urban and rural areas, and a potentially inadequate billing system in some Canadian provinces [2].
A survey conducted in 2021 indicated that over 50% of Canadian allergists (52.2%) offer OIT, mainly for peanut allergy. However, significant barriers to expanding OIT practice were reported, including lack of efficacy data, lack of support staff and clinic space, and concerns about increased OFCs [50]. Clinicians not offering OIT cited concerns about safety, after-hours support, efficacy, medicolegal risk, and long-term practice implications as major obstacles. Qualitative assessment revealed concerns about practical challenges associated with OIT, the need for increased safety and efficacy data, and the desire for OIT guidelines and training. Access to OIT in underserved areas will require collaboration between different healthcare professionals.
Milk and egg ladders: a modified form of OIT
Cow’s milk and egg are among the most common food allergies in young children. Although milk and egg allergies have historically been regarded to have a good prognosis, with many children outgrowing these allergies in childhood, evidence suggests that the rate of resolution may be slowing over time, with only 50% resolution by 5–6 years of age and increasing persistence of these allergies into adolescence or adulthood [51, 52]. A recent US population-level study found that Black and Hispanic patients, as well those with non-cutaneous symptoms, were less likely to outgrow cow’s milk allergy than White patients or those with cutaneous symptoms [53].
There is increasing recognition that a subset of children with egg and milk allergy may tolerate baked/processed forms of milk and egg. Observational studies have found that patients who incorporated baked products in their diet were more likely to outgrow their allergy [54, 55]. This has led to the hypothesis that baked products could increase the odds of developing tolerance to the raw food, while being a safer approach than OIT with the raw product [56]. However, it is critical to recognize that this has never been demonstrated in a randomized trial. Observational trials are at very high risk of bias since those patients who introduced baked goods are likely to be those with milder allergies.
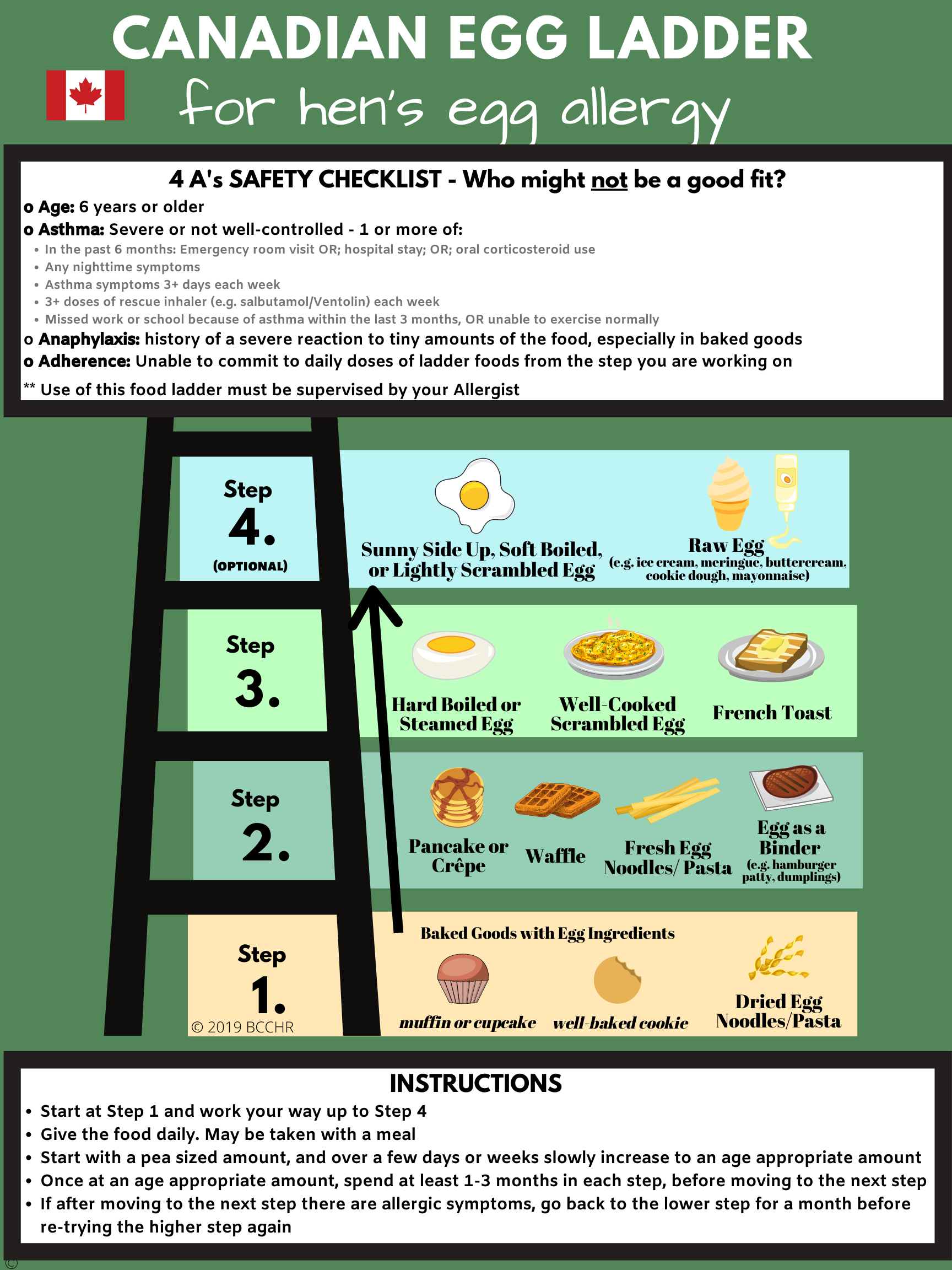
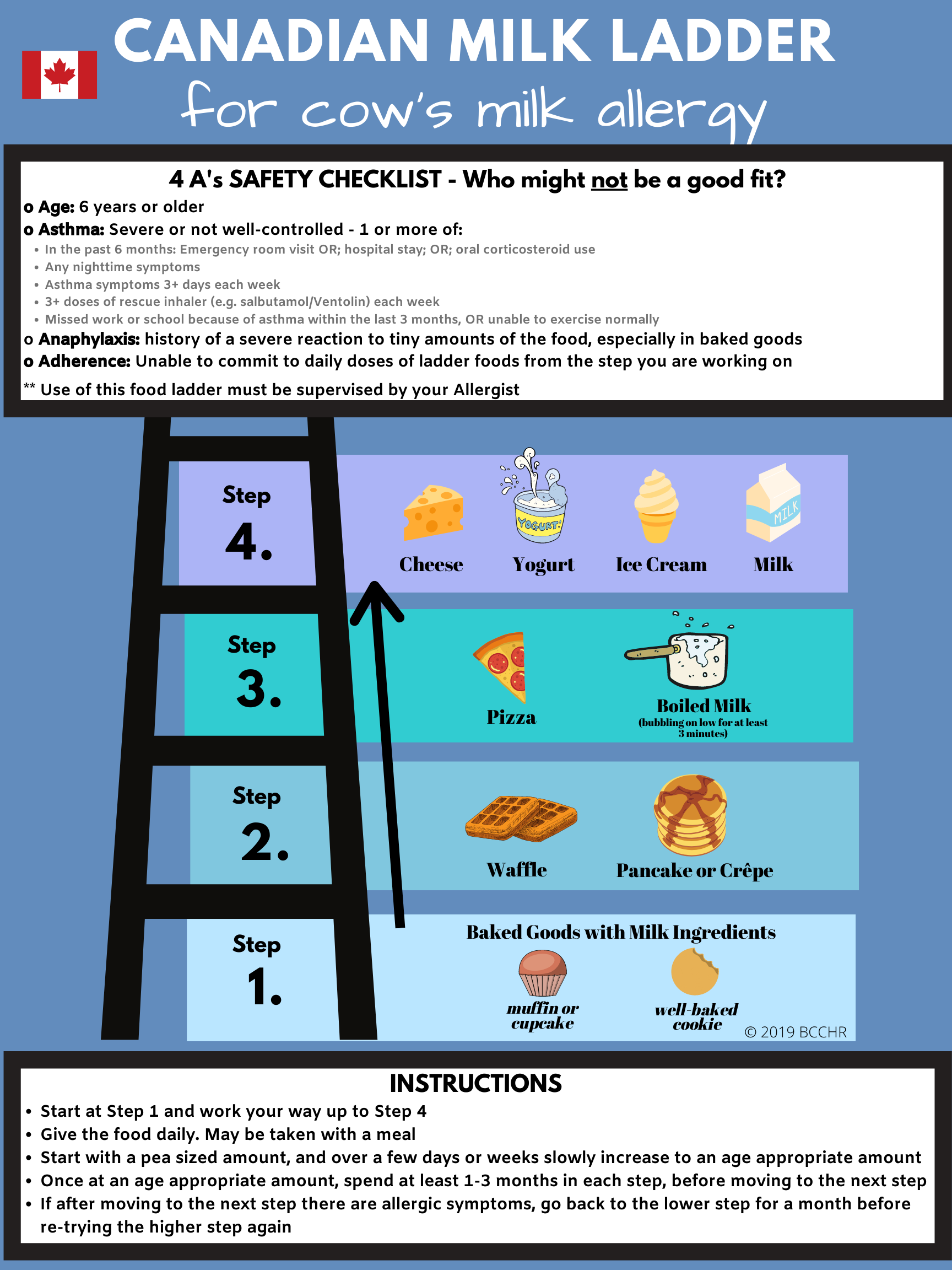
Food ladders were tools initially designed to guide patients with non-IgE-mediated food allergy through a home-based gradual, stepwise introduction of increasing allergenic forms of milk and egg (i.e., from extensively heated forms, such as baked goods [e.g., biscuits, muffins], to less processed products [e.g., yogurt or ice cream]) [57]. While originally designed to allow home reintroduction without the need for in-clinic OFCs, food ladders have more recently been proposed as a modified form of OIT to facilitate the development of natural tolerance to allergenic foods such as milk and egg [58] (see examples of food ladders in Figs. 2 and 3). A recent Canadian study found food ladders to be safe in children with IgE-mediated allergies to cow’s milk and/or egg, with participants tolerating a larger range of foods with food ladder use compared to baseline [59]. If food ladders are used for the purpose of facilitating the development of natural tolerance, they should be recognized as a modified form of OIT, carrying the same risks as traditional OIT. As such, food ladders should be administered by well-trained and experienced healthcare professionals with the necessary expertise in food allergy and anaphylaxis management, performance of OFCs, and careful selection of patients for food immunotherapy [60]. Failure to recognize that food ladders are being used as OIT can lead to a false sense of safety.

Adapted from: Chomyn A, et al. Allergy Asthma Clin Immunol. 2021;17(1):83 [58]. Creative Commons license: https://creativecommons.org/licenses/by/4.0/ The image has been updated to include the 4 A’s safety checklist. The Canadian egg ladder is available at: https://www.bcchr.ca/sites/default/files/group-food-allergy-treatment/_canadian-egg-ladder_sept-15.png Accessed September 6, 2024
Canadian egg ladder [58].

Adapted from: Chomyn A, et al. Allergy Asthma Clin Immunol. 2021;17(1):83 [58]. Creative Commons license: https://creativecommons.org/licenses/by/4.0/ The image has been updated to include the 4 A’s safety checklist. The Canadian milk ladder is available at: https://www.bcchr.ca/sites/default/files/group-food-allergy-treatment/canadian-milk-ladder.png Accessed September 6, 2024
Canadian milk ladder [58].
Appropriate patient selection for home-based egg and milk ladders is paramount. Experts have recently proposed a food ladder safety checklist to assist with patient selection using “4 A’s” based on available evidence for food ladders, including Age, active or poorly controlled Asthma, history of Anaphylaxis, and Adherence (see Figs. 2 and 3) [60]. Allergists may decline or delay offering food ladders while optimizing any modifiable factors, such as asthma, or may opt for an alternative dietary advancement therapy such as traditional OIT. Similar to traditional OIT, the decision to start a patient on a food ladder should be based on shared decision-making between the specialist, patient and caregiver, and therapy should be personalized to each individual patient/family.
Key considerations for non-allergist clinicians
Pediatricians, family physicians and other healthcare professionals working in the pediatric and family practice settings can play a key role in identifying patients with IgE-mediated food allergies who may be appropriate for OIT and who could benefit from referral to an allergist.
There are no consensus criteria to select patients for whom OIT could be proposed. Several factors should be considered such as patient age (i.e., OIT is safer and more effective in younger children), the natural evolution of the food allergy, the presence of comorbidities that may be contraindications for OIT (e.g., severe uncontrolled asthma [absolute contraindication], EoE [relative contraindication]), the patient’s experience (e.g., the burden of food allergy and impact on QoL), and the patient’s/family’s ability to understand the risks and benefits of therapy, adhere to the treatment protocol and manage possible adverse reactions to therapy. As mentioned earlier, families of infants who have failed primary prevention of food allergy (see Primary Prevention of Food Allergy: Beyond Early Introduction article in this supplement [36]) should be provided with infant OIT as a management option [60] and should be referred to an allergist if they are interested in pursuing this form of therapy.
Pediatricians and family physicians can also play an important role in the prevention and management of side effects of OIT as they can often be the first point of contact for patients experiencing an adverse reaction to therapy (see Table 3 for management strategies) [61]. Children undergoing OIT and their parents should be made aware of the possible occurrence of adverse events and how to treat these events. It is therefore important for pediatricians and family physicians to reinforce education received by the allergist and to ensure that families are equipped with an epinephrine auto-injector as well as a clear plan or flow sheet on how to manage at-home reactions, when to hold/reduce OIT doses (e.g., during a viral illness) and when to administer epinephrine (see Fig. 4) [21].

Flow sheet for parents–daily dose instructions and side effect management. Figure reproduced with permission from Dr. Lianne Soller on behalf of the Canadian Preschool Peanut Oral Immunotherapy (CPP-OIT) project
In cases of acute reactions, a possible error by clinicians in the emergency department is to recommend full discontinuation of OIT doses while waiting to see the allergist. Ideally, doses should be reduced but not stopped since this can lead to loss of protection.
Finally, in regions with no access to an allergist, primary-care providers should seek partnership with allergists from urban centers to establish local protocols that allow for the early initiation of OIT in their patients.
Future/emerging therapies
In addition to the expanding practice of OIT, there are other emerging therapies for the treatment of food allergy including sublingual immunotherapy (SLIT) and epicutaneous immunotherapy (EPIT). SLIT and EPIT consist of daily application of very small amounts of the allergen under the tongue with dissolvable tablets or liquid allergen extracts (SLIT) or on the skin with a patch device (EPIT). OIT has been the most studied form of food allergy treatment to date but, as side effects with OIT are common, SLIT and EPIT have been proposed as safer routes of administration with fewer adverse reactions. A recent placebo-controlled RCT found clinically significant desensitization with peanut SLIT compared to placebo in children aged 1–4 years with peanut allergy [62]. Side effects were similar between the SLIT and placebo groups, and no reactions required epinephrine. While SLIT may be safer than OIT (i.e., less side effects and less risk of epinephrine use), its efficacy may be slightly lower. In the above-mentioned RCT, 60% and 48% of peanut SLIT participants demonstrated desensitization and sustained unresponsiveness, respectively, compared to no placebo participants [62]. Higher rates of desensitization and sustained unresponsiveness are typically seen with OIT. Recently, an initial phase of multi-food SLIT using fresh food solutions (given the lack of Health Canada approved products) was used in a real-world Canadian study as a means to bypass OIT buildup in older children and adolescents for whom OIT is considered to be of higher risk [63]. None of the patients had severe reactions during SLIT, and 70% completed the low-dose OFC without any symptoms, allowing them to bypass OIT build-up and go directly from SLIT to OIT maintenance.
Emerging evidence also suggests that EPIT is safe and effective for the treatment of food allergy, as demonstrated in a recent phase 3 RCT that found 12 months of EPIT to be superior to placebo in desensitizing peanut-allergic children aged 1–3 years to peanut and a low rate of treatment-related anaphylaxis (1.6% in the EPIT group and none in the placebo group) [64]. Biologics, such as omalizumab (an anti-IgE monoclonal antibody that was first approved to treat allergic asthma), are also being studied as adjuvant treatment during OIT to reduce the risk of severe reactions [48, 65]. CSACI guidelines suggest that omalizumab as an off-label adjunct to OIT could be considered in more challenging cases to decrease the risk of anaphylaxis and accelerate treatment [2]. In February 2024, the Food and Drug Administration (FDA) approved omalizumab for reducing allergic reactions, including anaphylaxis, resulting from accidental exposure to one or more foods in individuals ≥ 1 year of age with IgE-mediated food allergies [66]. This approval was based on the initial stage of the OUtMATCH trial which showed that a 16-to-20-week course of omalizumab increased the amount of peanut, tree nuts, egg, milk and wheat that multi-food allergic children could consume without a moderate or severe allergic reaction [67]. The second stage of OUtMATCH will compare omalizumab monotherapy to omalizumab combined with OIT in patients with multi-food allergies [68]. Health Canada has not approved omalizumab for treatment of food allergy.
Currently, most OIT is supervised by an allergist in clinic, but there are reports of home-based OIT as an option for select patients. A case series reported by Chua et al. showed that home-based OIT could be offered to low-risk preschoolers during the coronavirus disease (COVID-19) pandemic [69]. Nine preschoolers with a history of mild allergic reactions to peanut underwent home-based peanut OIT. Eight (88.9%) completed the build-up phase at home in 11–28 weeks, tolerating a daily maintenance dose of 320 mg of peanut protein. Symptoms were common, but mild to moderate: six patients (75.0%) reported urticaria, three (33.3%) reported gastrointestinal tract symptoms, and one (14.3%) reported oral pruritis. None of the patients developed anaphylaxis, required epinephrine, or attended emergency services related to OIT. One or two virtual follow-up visits were completed per patient during the build-up phase.
Conclusions
OIT is a safe and effective treatment option for IgE‐mediated food allergy. Current Canadian, patient-centred, clinical practice guidelines recommend OIT for patients with IgE-mediated food allergy wishing to receive it, provided that there are no contraindications to therapy and that patients and caregivers clearly understand the benefits and risks of therapy. Shared decision-making between the patient, family and allergist are imperative before initiating OIT.
OIT is likely to become a more routine, standard therapeutic option in food allergy management in the future, but strategies are needed to address disparities in access to this form of therapy across Canada. Further research is needed on the long-term efficacy of OIT, and international consensus on safety reporting for OIT is required to facilitate the development of personalized protocols that improve safety outcomes.
Availability of data and materials
Data sharing not applicable to this article as no datasets were generated or analyzed during the development of this review.
Abbreviations
- ACE:
-
Angiotensin-converting enzyme
- CI:
-
Confidence interval
- CPP-OIT:
-
Canadian Preschool Peanut Oral Immunotherapy
- CSACI:
-
Canadian Society of Allergy and Immunology
- COVID-19:
-
Coronavirus disease
- EAACI:
-
European Academy of Allergy and Clinical Immunology
- EoE:
-
Eosinophilic esophagitis
- EPIT:
-
Epicutaneous immunotherapy
- GA2LEN:
-
Global Allergy and Asthma European Network
- IgE:
-
Immunoglobulin E
- IgG4:
-
Immunoglobulin G4
- NSAIDs:
-
Non-steroid anti-inflammatory drugs
- OFC:
-
Oral food challenge
- OIT:
-
Oral immunotherapy
- QoL:
-
Quality of life
- RCT:
-
Randomized controlled trial
- RR:
-
Risk ratio
- SABA:
-
Short-acting beta2-agonist
- SLIT:
-
Sublingual immunotherapy
References
Bégin P, Waserman S, Protudjer JLP, Jeimy S, Watson W. Immunoglobulin E (IgE)-mediated food allergy. Allergy Asthma Clin Immunol. 2024;20(Suppl 3):75.
Bégin P, Chan ES, Kim H, Wagner M, Cellier MS, Favron-Godbout C, et al. CSACI guidelines for the ethical, evidence-based and patient-oriented clinical practice of oral immunotherapy in IgE-mediated food allergy. Allergy Asthma Clin Immunol. 2020;16:20.
Phelps A, Bruton K, Grydziuszko E, Koenig JFE, Jordana M. The road toward transformative treatments for food allergy. Front Allergy. 2022;3: 826623.
Nurmatov U, Dhami S, Arasi S, Pajno GB, Fernandez-Rivas M, Muraro A, et al. Allergen immunotherapy for IgE-mediated food allergy: a systematic review and meta-analysis. Allergy. 2017;72(8):1133–47.
de Silva D, Rodríguez Del Río P, de Jong NW, et al. GA2LEN Food Allergy Guidelines Group. Allergen immunotherapy and/or biologicals for IgE-mediated food allergy: a systematic review and meta-analysis. Allergy. 2022;77(6):1852–1862.
Abrams EM, Erdle SC, Cameron SB, Soller L, Chan ES. How to Incorporate Oral Immunotherapy into Your Clinical Practice. Curr Allergy Asthma Rep. 2021;21(4):30.
Vickery BP, Berglund JP, Burk CM, Fine JP, Kim EH, Kim JI, et al. Early oral immunotherapy in peanut-allergic preschool children is safe and highly effective. J Allergy Clin Immunol. 2017;139(1):173-181.e8.
PALISADE Group of Clinical Investigators; Vickery BP, Vereda A, Casale TB, Beyer K, du Toit G, Hourihane JO, et al. AR101 Oral Immunotherapy for Peanut Allergy. N Engl J Med. 2018;379(21):1991–2001.
Jones SM, Kim EH, Nadeau KC, Nowak-Wegrzyn A, Wood RA, Sampson HA, et al. Immune Tolerance Network. Efficacy and safety of oral immunotherapy in children aged 1–3 years with peanut allergy (the Immune Tolerance Network IMPACT trial): a randomised placebo-controlled study. Lancet. 2022;399(10322):359–71.
Chinthrajah RS, Cao S, Dunham T, Sampath V, Chandra S, Chen M, Sindher S, Nadeau K. Oral immunotherapy for peanut allergy: the pro argument. World Allergy Organ J. 2020;13(8): 100455.
Kaman K, Dhodapkar M, Shabanova V, McCollum S, Factor J, Leeds S. Validated anxiety assessments among pediatric patients with peanut allergy on oral immunotherapy. Ann Allergy Asthma Immunol. 2023;130(5):657–63.
Cao S, Borro M, Alonzi S, Sindher S, Nadeau K, Chinthrajah RS. Improvement in health-related quality of life in food-allergic patients: a meta-analysis. J Allergy Clin Immunol Pract. 2021;9(10):3705–14.
Epstein-Rigbi N, Goldberg MR, Levy MB, Nachshon L, Elizur A. Quality of life of food-allergic patients before, during, and after oral immunotherapy. J Allergy Clin Immunol Pract. 2019;7(2):429-436.e2.
Burks AW, Jones SM, Wood RA, Fleischer DM, Sicherer SH, Lindblad RW, et al. Consortium of food allergy research (CoFAR). Oral immunotherapy for treatment of egg allergy in children. N Engl J Med. 2012;367(3):233–43.
Soller L, Abrams EM, Carr S, Kapur S, Rex GA, Leo S, et al. First real-world effectiveness analysis of preschool peanut oral immunotherapy. J Allergy Clin Immunol Pract. 2021;9(3):1349-1356.e1.
Chua GT, Soller L, Kapur S, McHenry M, Rex GA, Cook VE, et al. Real-world safety and effectiveness analysis of low-dose preschool sesame oral immunotherapy. J Allergy Clin Immunol Glob. 2023;3(1): 100171.
Grzeskowiak LE, Tao B, Knight E, Cohen-Woods S, Chataway T. Adverse events associated with peanut oral immunotherapy in children—a systematic review and meta-analysis. Sci Rep. 2020;10(1):659.
Zhu R, Robertson K, Protudjer JLP, Macikunas A, Kim R, Jeimy S, Kim H. Impact of age on adherence and efficacy of peanut oral-immunotherapy using a standardized protocol. Pediatr Allergy Immunol. 2021;32(4):783–6.
Chu DK, Wood RA, French S, Fiocchi A, Jordana M, Waserman S, Brożek JL, Schünemann HJ. Oral immunotherapy for peanut allergy (PACE): a systematic review and meta-analysis of efficacy and safety. Lancet. 2019;393(10187):2222–32.
Kansen HM, Le TM, Knulst AC, Gorissen DMW, van der Ent CK, Meijer Y, van Erp FC. Three-year follow-up after peanut food challenges: accidental reactions in allergic children and introduction failure in tolerant children. J Allergy Clin Immunol. 2020;145(2):705-707.e7.
Soller L, Abrams EM, Carr S, Kapur S, Rex GA, Leo S, et al. First real-world safety analysis of preschool peanut oral immunotherapy. J Allergy Clin Immunol Pract. 2019;7(8):2759-2767.e5.
Erdle SC, Cook VE, Cameron SB, Yeung J, Kapur S, McHenry M, et al. Real-world safety analysis of preschool tree nut oral immunotherapy. J Allergy Clin Immunol Pract. 2023;11(4):1177–83.
Boursiquot JN, Gagnon R, Quirt J, Ellis AK. Allergen immunotherapy. Allergy Asthma. Clin Immunol. 2024;20(Suppl 3):66.
Kovaltchouk U, Jeimy S, Soller L, Robertson K, Abrams EM, Cameron SB, Kim H, Chan ES. Comparing the risk of anaphylaxis requiring epinephrine in oral immunotherapy and subcutaneous immunotherapy: a review of recent Canadian real-world literature. J Allergy Clin Immunol Glob. 2023;2(2): 100080.
Erdle SC, Carr S, Chan ES, Robertson K, Watson W. Eosinophilic esophagitis. Allergy Asthma. Clin Immunol. 2024;20(Suppl 3):72.
Lucendo AJ, Arias A, Tenias JM. Relation between eosinophilic esophagitis and oral immunotherapy for food allergy: a systematic review with meta-analysis. Ann Allergy Asthma Immunol. 2014;113(6):624–9.
Barbosa AC, Castro FM, Meireles PR, Arruda LK, Cardoso SR, Kalil J, Yang AC. Eosinophilic esophagitis: latent disease in patients with anaphylactic reaction to cow’s milk. J Allergy Clin Immunol Pract. 2018;6(2):451–6.
Goldberg MR, Nachston L, Levy MB, Elizur A, Katz Y. Risk factors and treatment outcomes for oral immunotherapy-induced gastrointestinal symptoms and eosinophilic responses (OITIGER). J Allergy Clin Immunol Pract. 2020;8(1):125–31.
Epstein-Rigbi N, Elizur A, Levy MB, Nachshon L, Koren Y, Shalem Z, et al. Treatment of oral immunotherapy-associated eosinophilic esophagitis. J Allergy Clin Immunol Pract. 2023;11(4):1303–5.
Wright BL, Fernandez-Becker NQ, Kambham N, Purington N, Cao S, Tupa D, et al. Gastrointestinal eosinophil responses in a longitudinal, randomized trial of peanut oral immunotherapy. Clin Gastroenterol Hepatol. 2021;19(6):1151-1159.e14.
Wilson BE, Meltzer EC, Wright BL. Ethical implications of continuing oral immunotherapy after the development of eosinophilic esophagitis. J Allergy Clin Immunol Pract. 2023;11:S2213–S2198.
Avinashi V, Al Yarubi Z, Soller L, Lam G, Chan ES. Oral peanut immunotherapy acutely unmasking eosinophilic esophagitis with an esophageal stricture. Ann Allergy Asthma Immunol. 2021;127(6):691–2.
Chua GT, Chan ES, Invik R, Soller L, Avinashi V, Erdle SC, et al. How we manage gastrointestinal symptoms during oral immunotherapy through a shared decision-making process—a practical guide for the community practitioner. J Allergy Clin Immunol Pract. 2023;11(4):1049–55.
Mori F, Giovannini M, Barni S, Jiménez-Saiz R, Munblit D, Biagioni B, et al. Oral immunotherapy for food-allergic children: a pro-con debate. Front Immunol. 2021;12: 636612.
Morris E, Protudjer JLP, Jeimy S, Edgerley S, Rondilla N, Robertson K, Zhu R, Kim H. Evening ingestion as a potential reaction cofactor during peanut oral immunotherapy in children. J Allergy Clin Immunol Pract. 2023;11(6):1964-1966.e2.
Chan ES, Abrams EM, Mack DP, Protudjer JLP, Watson W. Primary prevention of food allergy: beyond early introduction. Allergy Asthma Clin Immunol. 2024;20(Suppl 3):71.
Fleischer DM, Chan ES, Venter C, Spergel JM, Abrams EM, Stukus D, et al. A consensus approach to the primary prevention of food allergy through nutrition: guidance from the American academy of allergy, asthma, and immunology; American college of allergy, asthma, and immunology; and the Canadian society for allergy and clinical immunology. J Allergy Clin Immunol Pract. 2021;9(1):22-43.e4.
Togias A, Cooper SF, Acebal ML, Assa’ad A, Baker JR, Beck LA, et al. Addendum guidelines for the prevention of peanut allergy in the United States: report of the National Institute of Allergy and Infectious Diseases-sponsored expert panel. Ann Allergy Asthma Immunol. 2017;118(2):166–73.
Abrams EM, Orkin J, Cummings C, Blair B, Chan ES. Dietary exposures and allergy prevention in high-risk infants. Paediatr Child Health. 2021;26(8):504–5.
Peters RL, Allen KJ, Dharmage SC, Koplin JJ, Dang T, Tilbrook KP, et al. HealthNuts Study. Natural history of peanut allergy and predictors of resolution in the first 4 years of life: a population-based assessment. J Allergy Clin Immunol. 2015;135(5):1257–66.
Foong RX, Santos AF. Biomarkers of diagnosis and resolution of food allergy. Pediatr Allergy Immunol. 2021;32(2):223–33.
Soller L, Carr S, Kapur S, Rex GA, McHenry M, Cook VE, et al. Real-world peanut OIT in infants may be safer than non-infant preschool OIT, and equally effective. J Allergy Clin Immunol Pract. 2022;10(4):1113–6.
Demidova A, Drewitz KP, Kimkool P, Banjanin N, Barzylovich V, Botjes E, et al. COMFA Consortium. Core Outcome Set for IgE-mediated food allergy clinical trials and observational studies of interventions: International Delphi consensus study ‘COMFA.’ Allergy. 2024;79(4):977–89.
Lloyd M, Patel N, Munblit D, Tang MLK. Endpoints and outcomes after immunotherapy for food allergy: What is meaningful for patients? J Allergy Clin Immunol Pract. 2023;11(4):998–1007.
Shaker M, Chan ES, Protudjer JLP, Soller L, Abrams EM, Greenhawt M. The cost-effectiveness of preschool peanut oral immunotherapy in the real-world setting. J Allergy Clin Immunol Pract. 2021;9(7):2876–84.
Galvin AD, Vereda A, Rodríguez del Río P, Muraro A, Jones C, Ryan R, et al. Children and caregiver proxy quality of life from peanut oral immunotherapy trials. Clin Transl Allergy. 2022;12(12): e12213.
Chua GT, Greenhawt M, Shaker M, Soller L, Abrams EM, Cameron SB, et al. The case for prompt salvage infant peanut oral immunotherapy following failed primary prevention. J Allergy Clin Immunol Pract. 2022;10(10):2561–9.
Pouessel G, Lezmi G. Oral immunotherapy for food allergy: translation from studies to clinical practice? World Allergy Organ J. 2023;16(2): 100747.
Pajno GB, Fernandez-Rivas M, Arasi S, Roberts G, Akdis CA, Alvaro-Lozano M, et al. EAACI allergen immunotherapy guidelines group. EAACI Guidelines on allergen immunotherapy: IgE-mediated food allergy. Allergy. 2018;73(4):799–815.
Mack DP, Soller L, Chan ES, Hanna MA, Terpstra C, Vander Leek TK, Bégin P. A high proportion of Canadian allergists offer oral immunotherapy but barriers remain. J Allergy Clin Immunol Pract. 2021;9(5):1902–8.
Wood RA, Sicherer SH, Vickery BP, Jones SM, Liu AH, Fleischer DM, et al. The natural history of milk allergy in an observational cohort. J Allergy Clin Immunol. 2013;131(3):805–12.
Sicherer SH, Wood RA, Vickery BP, Jones SM, Liu AH, Fleischer DM, et al. The natural history of egg allergy in an observational cohort. J Allergy Clin Immunol. 2014;133(2):492–9.
Warren CM, Agrawal A, Gandhi D, Gupta RS. The US population-level burden of cow’s milk allergy. World Allergy Organ J. 2022;15(4): 100644.
Kim JS, Nowak-Węgrzyn A, Sicherer SH, Noone S, Moshier EL, Sampson HA. Dietary baked milk accelerates the resolution of cow’s milk allergy in children. J Allergy Clin Immunol. 2011;128(1):125-131.e2.
Peters RL, Dharmage SC, Gurrin LC, Koplin JJ, Ponsonby AL, Lowe AJ, et al. HealthNuts study. The natural history and clinical predictors of egg allergy in the first 2 years of life: a prospective, population-based cohort study. J Allergy Clin Immunol. 2014;133(2):485–91.
Nowak-Wegrzyn A, Fiocchi A. Rare, medium, or well done? The effect of heating and food matrix on food protein allergenicity. Curr Opin Allergy Clin Immunol. 2009;9(3):234–7.
Luyt D, Ball H, Makwana N, Green MR, Bravin K, Nasser SM, Clark AT. Standards of Care Committee (SOCC) of the British Society for Allergy and Clinical Immunology (BSACI). BSACI guideline for the diagnosis and management of cow’s milk allergy. Clin Exp Allergy. 2014;44(5):642–72.
Chomyn A, Chan ES, Yeung J, Vander Leek TK, Williams BA, Soller L, et al. Canadian food ladders for dietary advancement in children with IgE-mediated allergy to milk and/or egg. Allergy Asthma Clin Immunol. 2021;17(1):83.
Chomyn A, Chan ES, Yeung J, Cameron S, Chua GT, Vander Leek TK, et al. Safety and effectiveness of the Canadian food ladders for children with IgE-mediated food allergies to cow’s milk and/or egg. Allergy Asthma Clin Immunol. 2023;19(1):94.
Chua GT, Chan ES, Yeung J, Cameron SB, Soller L, Williams BA, et al. Patient selection for milk and egg ladders using a food ladder safety checklist. Allergy Asthma Clin Immunol. 2022;18(1):51.
Sabouraud M, Biermé P, Andre-Gomez SA, Villard-Truc F, Corréard AK, Garnier L, et al. Oral immunotherapy in food allergies: a practical update for pediatricians. Arch Pediatr. 2021;28(4):319–24.
Kim EH, Bird JA, Keet CA, Virkud YV, Herlihy L, Ye P, et al. Desensitization and remission after peanut sublingual immunotherapy in 1- to 4-year-old peanut-allergic children: a randomized, placebo-controlled trial. J Allergy Clin Immunol. 2024;153(1):173–81.
Soller L, Williams BA, Mak R, Wong T, Erdle SC, Chomyn A, et al. Safety and effectiveness of bypassing oral immunotherapy buildup with an initial phase of sublingual immunotherapy for higher-risk food allergy. J Allergy Clin Immunol Pract. 2024;12(5):1283-1296.e2.
Greenhawt M, Sindher SB, Wang J, O’Sullivan M, du Toit G, Kim EH, et al. Phase 3 trial of epicutaneous immunotherapy in toddlers with peanut allergy. N Engl J Med. 2023;388(19):1755–66.
MacGinnitie AJ, Rachid R, Gragg H, Little SV, Lakin P, Cianferoni A, et al. Omalizumab facilitates rapid oral desensitization for peanut allergy. J Allergy Clin Immunol. 2017;139(3):873-881.e8.
FDA Approves First Medication to Help Reduce Allergic Reactions to Multiple Foods After Accidental Exposure. News Release. FDA. February 16, 2024. Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-medication-help-reduce-allergic-reactions-multiple-foods-after-accidental Accessed April 30, 2024.
Wood RA, Togias A, Sicherer SH, Shreffler WG, Kim EH, Jones SM, et al. Omalizumab for the treatment of multiple food allergies. N Engl J Med. 2024;390(10):889–99.
Wood RA, Chinthrajah RS, Rudman Spergel AK, Babineau DC, Sicherer SH, Kim EH, et al. OUtMATCH study team. Protocol design and synopsis: omalizumab as Monotherapy and as Adjunct Therapy to Multiallergen OIT in Children and Adults with Food Allergy (OUtMATCH). J Allergy Clin Immunol Glob. 2022;1(4):225–32.
Chua GT, Chan ES, Soller L, Cook VE, Vander Leek TK, Mak R. Home-based peanut oral immunotherapy for low-risk peanut-allergic preschoolers during the COVID-19 pandemic and beyond. Front Allergy. 2021;2: 725165.
Acknowledgements
The authors thank Julie Tasso for her editorial services and assistance in the preparation of this manuscript.
About this supplement
This article has been published as part of Allergy, Asthma & Clinical Immunology, Volume 20 Supplement 03, 2024: Practical Guide for Allergy and Immunology in Canada 2024. The full contents of the supplement are available at https://biomedcentral-aacijournal.publicaciones.saludcastillayleon.es/articles/supplements/volume-20-supplement-3.
Funding
Publication of this supplement has been supported by ALK, Biocryst, CSL Behring, GSK, Miravo, Medexus, Novartis, Stallergenes Greer, and Takeda. The supporters had no involvement in the writing, development or review of this manuscript.
Author information
Authors and Affiliations
Contributions
The authors confirm contribution to the paper as follows: conception and design: MM; acquisition of data: MM, PB, ESC, ML; analysis and interpretation of data: MM, PB, ESC, ML, HK; drafting of manuscript: MM; critical revision and editing of manuscript: MM, PB, ESC, ML, HK. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval and consent to participate are not applicable to this review article.
Consent for publication
Not applicable.
Competing interests
Dr. Mary McHenry has received consulting fees and honoraria from Sanofi Genzyme and Medexus, and is on the Board of Directors for CAAIF. Dr. Philippe Bégin has received consulting fees and honoraria from ALK, Astra Zeneca, Sanofi, Bausch Health, Pfizer. He is also a clinical trial investigator with DBV Technologies (Viaskin Patch), Regeneron, Novartis, ALK, and Sanofi. He is on the Board of Directors of the CSACI, AAIQ and CAAIF and medical advisor to Food Allergy Canada. Dr. Edmond Chan has received research support from DBV Technologies; has been a member of advisory boards for Pfizer, Miravo, Medexus, Leo Pharma, Kaleo, DBV, AllerGenis, Sanofi Genzyme, Bausch Health, Avir Pharma, AstraZeneca, ALK, Alladapt; was co-lead of the CSACI oral immunotherapy guidelines; is on the Executive of the CSACI (Canadian Society of Allergy and Clinical Immunology); is on the Executive of the CPS (Canadian Paediatric Society) Allergy Section; and is a member of the healthcare advisory board for Food Allergy Canada. Dr. Meriem Latrous has received consulting fees and honoraria from Sanofi, ALK, Pfizer, Miravo, and Bausch Health. Dr. Harold Kim has received honoraria and/or consulting fees from ALK, AstraZeneca, Bausch Health, CSL Behring, GSK, Miravo, Novartis, Medexus, Pfizer, Sanofi, Shire, Takeda.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
{kind=link}
Cite this article
McHenry, M., Bégin, P., Chan, E.S. et al. Food oral immunotherapy. Allergy Asthma Clin Immunol 20 (Suppl 3), 82 (2024). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s13223-025-00948-5
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s13223-025-00948-5